

Health workers worry fear, distrust complicate COVID-19 tracing in Minnesota’s communities of color

Go Deeper.
Create an account or log in to save stories.
Like this?
Thanks for liking this story! We have added it to a list of your favorite stories.
For months, as they’ve tracked the coronavirus’ creep across the state, epidemiologists at the Minnesota Department of Health have quietly worried about the impacts of a single paragraph they’re required to read at the end of every case interview.
It’s an opt-in, intended to let a patient know how their contact information will be shared with law enforcement.
But the health workers fear it has had an unintended chilling effect on the critical work of testing and tracing positive COVID-19 cases to stop the spread of the virus in some of Minnesota’s most vulnerable communities — a concern they’ve raised repeatedly to the highest levels of state government.
Those fears played out for one Minnesota woman, Lizeth, in early April, when COVID-19 was still a relatively new and baffling disease.
Turn Up Your Support
MPR News helps you turn down the noise and build shared understanding. Turn up your support for this public resource and keep trusted journalism accessible to all.
She had dropped her husband off at a local emergency room after he’d battled three weeks of fevers, a cough and extreme fatigue. He was quickly diagnosed with COVID-19. She wasn’t allowed to be with him in the hospital.
He was alone, battling this brand-new illness in intensive care, when his doctor called Lizeth, an undocumented immigrant from El Salvador who asked that MPR News only identify her by her middle name, to tell her that her husband was going to be intubated.
“He said my husband’s health was declining, and they didn’t see improvement with the treatment,” she said through an interpreter.
She feared she would never see him again.
Then, a case investigator from the state Health Department called Lizeth to ask her a battery of questions about her husband — where he had been, how he might have gotten sick, who he had been in contact with — the first step in the state’s multipronged effort to track and trace the virus’s spread, patient by patient.
In the middle of the call, the case investigator asked her a question that sent her into a spiral of anxiety: Would she agree to share her husband’s address with the state Department of Public Safety?
Reading from a script, the case investigator told Lizeth that if she did, “the types of first responders who will be told your address will be ambulance services, police, sheriff, fire, probation and parole agents, and sometimes federal agents such as the FBI or Immigration and Customs Enforcement or ICE.”
Giving Lizeth’s address to the Department of Public Safety would allow first responders to know if they needed to wear personal protective equipment if called to her house, to protect themselves against COVID-19.
At the time, in early April, PPE was in short supply, and being rationed — so Gov. Tim Walz signed an executive order requiring the state Health Department to share with its Public Safety Department the addresses of people who had tested positive for the virus, verified during the COVID-19 case investigation process.
But Lizeth said the question made her furious.
“I thought, ‘I’m not sharing my information with anybody,’” she said. For more than a decade, she’d lived under the radar in this country, careful to keep her personal information close, for fear of being deported by law enforcement.

“Even though I was scared about my husband’s situation, it’s the call that scared me the most,” said Lizeth. “Imagine: The day they called me to say this, was the day my husband had been intubated. It was too much.”
Already wary of the government, Lizeth refused to verify her address for the case investigator. She said she had another call coming in, and abruptly hung up.
Later, she said, she warned friends in her community to be careful with the information they shared if the Health Department called.
Case investigators at the department say they’ve seen Lizeth’s story replicated throughout the course of the pandemic. They say asking people to share personal information with law enforcement discourages them — and particularly anyone who is wary of the police or government — from fully participating in interviews, or getting tested for COVID-19 in the future.
And that hinders public health workers’ ability to gather accurate information that helps them piece together how the virus is spreading, and inform key decisions on how to contain it.
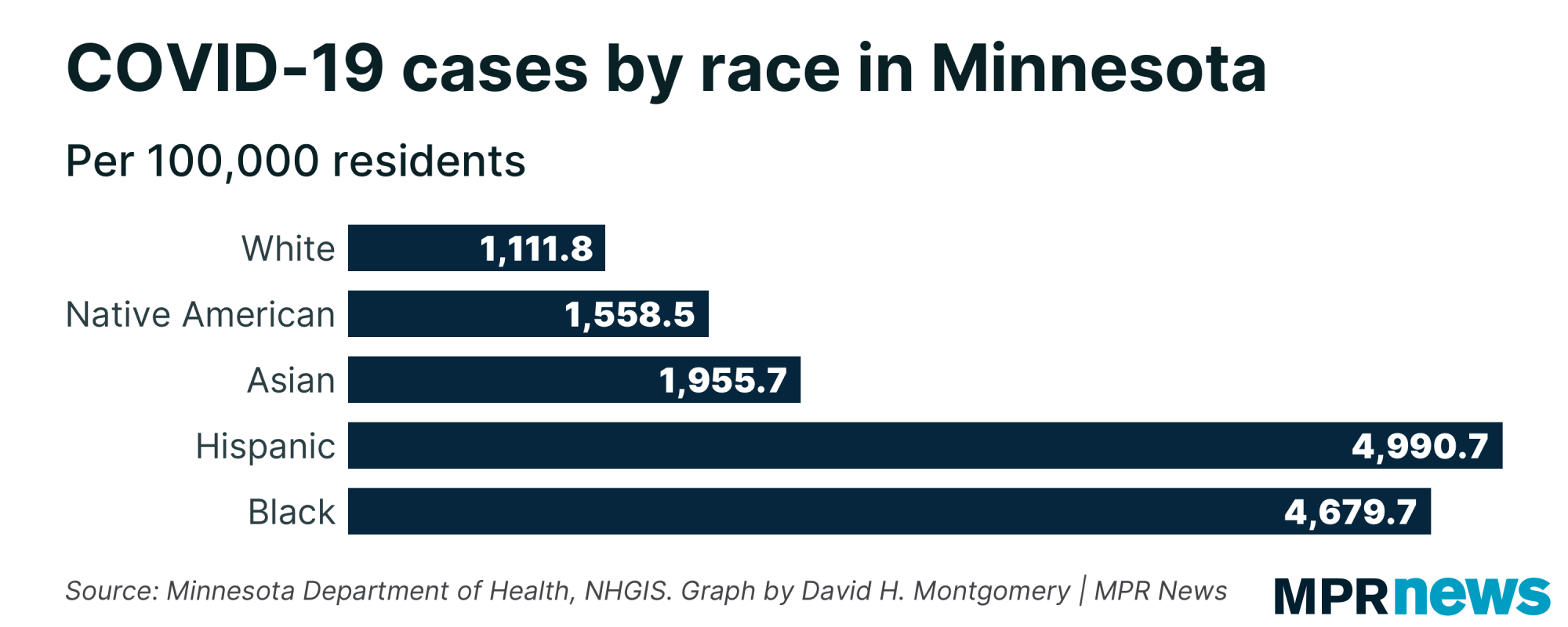
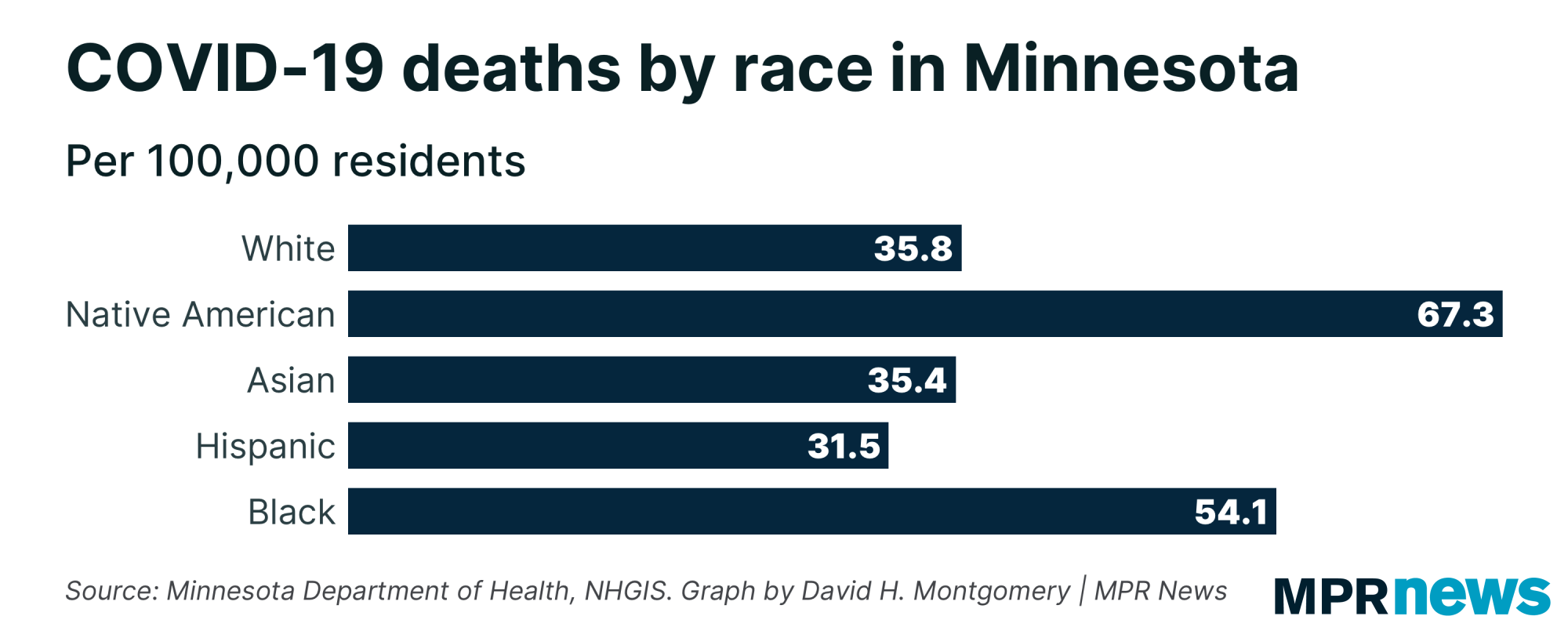
Collecting that information is especially important among Minnesota’s communities of color, who are at a higher risk of contracting the virus, being hospitalized for it and dying from it.
Case investigation, then contact tracing
When a person in Minnesota tests positive for COVID-19, they are first contacted by a case investigator from the Health Department, who gathers basic information to kickstart the contact tracing process, a key public health tool that helps the state better understand, and mitigate, the spread of the disease.
When COVID-19 patients don’t fully participate or provide inaccurate information, it has a ripple effect, said Mateo Frumholtz, an epidemiologist at the health department.
“We need to know that information just so we can call those other folks — family, friends — and tell them they were exposed to COVID-19,” he said.
“We want to talk you through what that means, how you can stay healthy and stay safe, and how you can keep other people healthy and safe. That is why it’s so important to give accurate information to us, and also to participate in this process to begin with.”
Protecting patient privacy is a core practice for infectious disease epidemiologists; to successfully track and contain diseases, they need patients to trust them with private information.
But in interviews, emails, a petition and other documents provided to MPR News, MDH epidemiologists and other Health Department employees involved in the state's COVID-19 response say the executive order that requires their department to share data with the state’s public safety department — Executive Order 20-34 — represents a breach of that trust, particularly among immigrants and communities of color, which suffer disproportionately from the ravages of COVID-19.
In the early days of the pandemic, when personal protective equipment was scarce and supply chains were disrupted, first responders and law enforcement groups lobbied the state for a system that would tell them if they’re being dispatched to a house with a COVID-positive patient. Addresses from the Health Department was one way to get that information.
In response to those concerns, Gov. Walz signed Executive Order 20-34 on April 10.
And since then, Health Department epidemiologists have at least four times in writing attempted to bring their own manifold concerns about the data sharing to the Walz administration.
Sharing data outside the Health Department, they worry, could lead to breaches or misuse. They also question the continued necessity of the order now, more than six months into the pandemic: The virus is so widespread, they argue, that any call could result in an exposure. Personal protective equipment, they say, is also much more accessible than it was in the spring.
But they are also concerned that the simple act of warning people that their information will be accessible to law enforcement, if they allow it, has hampered their efforts to track and isolate new cases, particularly in communities of color.
In mid-April, 61 Health Department employees working on the state’s COVID-19 response efforts took the unusual step of writing and signing a petition that crossed the desk of the state’s health commissioner, Jan Malcolm.
“Patient privacy is essential to the trust and confidence between staff at the Minnesota Department of Health and patients who test positive for reportable infectious disease,” they wrote. “Patient privacy cannot be ensured in this data sharing.”
The health workers say their petition was delivered to the governor’s office on April 15, five days after the data-sharing order was signed.
“We have … worked to obtain the best data by gaining the trust of the patients we interview. If mistrust exists between citizens and their government, we lose potential for quality data and our response to the COVID-19 pandemic is driven by that data,” the petition said.
According to Health Department spokesperson Michael Schommer, Malcolm is aware of and supportive of staff concerns around data sharing. Schommer said the commissioner has brought those concerns to the governor.
In a written statement, Walz spokesperson Teddy Tschann said the governor was also aware of the concerns.
“The pandemic poses many challenges that don’t have perfect solutions,” Tschann said. “Leading experts at state agencies often have a difference of opinion. It’s up to the governor to strike a balance when making decisions and do what he believes is in the best interest of Minnesota.”
In September, some of the health workers’ privacy concerns were realized, when the city of Minneapolis’ emergency communications team alerted the state that some addresses had been sent to them via unencrypted emails, in violation of the data sharing agreement between the health and public safety departments.
Department of Public Safety spokesperson Bruce Gordon said the errors were not deliberate, and that there was no evidence that the information had been misused. The Health Department has put a temporary hold on sharing new information with the Public Safety Department while the issue is resolved.
Urgent need to share data
Since Executive Order 20-34 was enacted, the Health Department has sent the addresses of newly confirmed COVID-19 patients to its counterparts in the state’s public safety department.
That information is shared with 911 dispatchers across the state, who have signed a confidentiality agreement, and only have access to addresses in their region.
When dispatchers connect first responders, police or other law enforcement to calls, houses where residents have tested positive for COVID-19 are flagged. First responders then know to assume they will come in contact with someone in the home who has the coronavirus.
“[The data sharing] is imperative to protect their health and safety during a time when personal protective equipment is in short supply,” according to an FAQ document about the executive order supplied by the state Department of Public Safety, which didn’t respond to requests for an interview about the impact of the order.
The DPS document goes on to say that there is a chance that federal agents, including immigration officials, might encounter that information if they alert 911 dispatchers when they are en route to a house, a courtesy that happens occasionally. In that case, the dispatcher would also tell the federal agents there’s an active coronavirus case at their destination.
The language about that data that Health Department investigators are required to read has changed several times since the executive order was enacted in April — in part to better explain how it will be shared with public safety departments.
In the spring, when Lizeth’s husband was sick, those warnings singled out ICE as a federal authority that might have access to their address and diagnosis.
But since then, mentions of ICE and the FBI have been dropped from the script, given the unlikely possibility that officers from those agencies would be given information about where COVID-19 patients live. It still mentions broader entities, such as federal law enforcement and probation and parole agents.
‘Shocked when that order was signed’
MPR News has found no evidence that the information the state Health Department shares with its public safety counterparts is being used in ways that are inconsistent with public health needs.
Nevertheless, the practice raised red flags among Health Department employees even before Walz signed the executive order.
“There was concern from the beginning, really at all levels of the response, from the people working on case investigation to our higher levels. It’s just ingrained in us in public health that we protect people’s private data,” said a longtime Health Department infectious disease epidemiologist, who did not want to give their name for fear of losing their job.
“If I write a phone number of a case on a Post-It note, and that’s all that’s on the Post-It note, I walk that over to the shredder,” the epidemiologist said. “A bunch of us were very shocked when that order was signed.”
But it wasn’t just the idea of sharing private data outside the realm of public health that shook the department’s COVID-19 response staff. It was the impact it could have on people like Lizeth that worried them.
In a series of emails from early April, as the Walz administration was hammering out the details of the executive order, the Health Department’s infectious disease and legal staff discussed these concerns and how to present them to public safety officials.
Primary among them: Whether undocumented immigrants or people who have a complicated history with law enforcement would agree to a case investigation interview if they were told their address would be shared with the state’s public safety department.
Disproportionate impacts
Case investigators say people of color — the very groups who are disproportionately affected by the coronavirus — are also less likely than white patients to consent to sharing their addresses with the Public Safety Department.
According to state Health Department data, nearly 40 percent of all Hispanic patients with COVID-19 who have been interviewed by the state have declined to confirm their addresses for the purposes of being shared with the public safety department.
Nearly 45 percent of Black patients have also declined to verify their addresses — and similar trends hold true for the state’s Asian and Indigenous populations. By contrast, only 27 percent of white patients have also declined.
Patients’ refusal to verify their addresses with case investigators doesn’t have an impact on the health department’s tallies of positive cases. The number and counties where patients who test positive are living, for instance, are gathered from other sources, such as health care providers and testing labs.

But it can have an impact on the information case investigators need to continue the work of contact tracing. In some cases, the question may prompt the patient to end the interview early. Or, in tightly knit communities, word will get out that the state is calling and asking to share addresses with law enforcement.
In those situations, other people who have been exposed to the virus may not pick up the phone at all when the health department calls.
That’s what Monica Hurtado, a community health organizer with the nonprofit Voices for Racial Justice, saw early in the pandemic when a coronavirus outbreak swept through far southwestern Minnesota and a Worthington meatpacking plant. Many infected workers were Hispanic.
At the time, Hurtado was helping leaders in communities of color there connect with agencies and the governor’s office on things like access to testing and workers’ rights.
“And I was getting calls from people saying, ‘Monica, this person has questions about COVID, they’re fearful of connecting with people at MDH.’ They got a call, but they hung up when they heard their information would be shared with first responders, with the police, with ICE,” said Hurtado.
Hurtado said she would reassure patients in the area that it was OK to talk to public health workers. But the fear persisted and spread through word of mouth, she said. In some cases, she said, people refused to pick up the phone at all when the Health Department called, hampering contact tracing in a community hit hard by the virus.
“We know the distrust is already there. People live in fear of ICE coming and doing raids. People don’t answer the door,” Hurtado said. “This executive order was not smart because it undermines the other great work the administration is doing.”
That dynamic played out the moment Lizeth hastily hung up the phone with the Health Department this spring.
In the days and weeks following, she warned friends in her community who had coronavirus to be cautious with the information they share with the Health Department.
“I tell them, ‘Be careful with the information that you share. You never know what’s going on with these people,’” said Lizeth.
And her husband, who stayed in the hospital for 16 days, eventually came home. Five months later, she said, he’s doing fine.